|
|||||||||||||||||
|
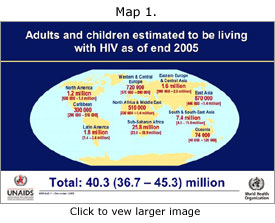
Despite evidence that prevention programs instituted some time ago are beginning to have an impact in some countries, the HIV/AIDS epidemic continues to grow. By 2005, the number of those infected had grown to more than 40 million, double the number in 1995. Previous success stories in Thailand and Uganda show potential to weaken as prevention programs have become less diligent. Globally, new infections among women, especially young women, continued to outpace those among men, - a stark reminder that gender inequity and violence against women fuel the epidemic. Life-saving drugs to prevent mother-to-child transmission of HIV have not been available to the hundreds of thousands of infants who have become needlessly infected at birth or through breastfeeding in the last year. According to UNAIDS and WHO, stigma and discrimination, whether actual or feared, remain perhaps the most difficult obstacles to prevention of HIV. |
|||||||||||||||||
A unified and global commitment to turning the tide on this disease is nonetheless building. This effort requires more resources and more effective use of resources devoted to research, prevention, care and treatment for those infected with and affected by the disease. Simultaneous and sustained expansion of prevention and treatment efforts are needed if the pace of the epidemic is to be slowed. Map 1. of current HIV/AIDS infections. This map is updated periodically at: www.unaids.org/EN/resources/epidemiology.asp |
|
||||||||||||||||
|
|||||||||||||||||
|
Global
Disparity Global trends of infection emerging from the HIV/AIDS pandemic: |
|||||||||||||||||
|
|||||||||||||||||
|
Women and
AIDS By the end of 2005, women accounted for nearly half of all people living with AIDS worldwide, and represent almost 60% of infections in sub-Saharan Africa. The impact of HIV on women is also growing in Eastern Europe, Central Asia and South and South-East Asia. Moreover, young women are several times more likely than young men to contract the disease through heterosexual contact. Worldwide, 62% of infected young people are girls, and that number soars to 77% in sub-Saharan Africa. A woman's vulnerability to the virus is attributable not only to biological differences, but also to deeply entrenched socio-economic inequalities that further compound her risk. Because 70% of the world's poor are women, women have fewer economic options. They are far more vulnerable because of absolute poverty to engage in transactional sex to pay for food, school fees and other necessities. They are also vulnerable to coercive or forced sex and often unable to negotiate condom use. One in three women world-wide have been affected by gender-based violence, but poor women are even more likely to be abused. Many women, particularly married women, cannot control the circumstances under which sex takes place. Research in several countries shows that for far too many young girls, the first sexual experience is coerced or forced. Married women are especially unable to negotiate sex or condom use with their husbands who may have extramarital partners. Some research indicates that married women are in fact more at risk for HIV than unmarried women because they are more frequently exposed to intercourse within marriage. HIV-positive women may transmit HIV to their children during pregnancy, in childbirth or through breastfeeding. Today, mother-to-child transmission (MTCT) of HIV is the primary mode of acquisition of HIV for the more than 2 million children living with HIV. While antiretroviral therapy significantly reduces the risk of MTCT of HIV, prevention coverage in the 30 African countries with the highest HIV prevalence is only 5 percent. As AIDS ravages families and communities, the burden of caring for ill family members rests mainly with women and girls - many of whom may be seriously ill themselves. A woman affected by HIV/AIDS is plunged further into poverty, losing the ability to provide for herself and her children. Combined with pervasive social stigma and the collapse of traditional family and support structures, HIV/AIDS is eroding the status of women in many countries.
|
|||||||||||||||||
|
Reasons
for Hope |
|||||||||||||||||
|
|||||||||||||||||